When intended parents begin a surrogacy journey, they carry more than hope. They carry years of longing, significant financial investment, and often the emotional weight of infertility or loss. So when conversations arise about prenatal care - especially if a surrogate shares that she plans to deliver with a midwife — it can bring up immediate questions.
Is it safe?
Isn’t IVF automatically high-risk?
Shouldn’t an OB be in charge?
These questions don’t come from distrust. They come from love and protection. And they deserve thoughtful, informed answers.
At the same time, it’s equally important to acknowledge something that can feel uncomfortable to say out loud: while intended parents are investing deeply in this journey, the surrogate is the one carrying the pregnancy and assuming the medical risk. The model of care she chooses matters — because it directly affects her body, her safety, and her birth experience.
Understanding what midwifery care actually looks like today can help bridge that gap.
What a Certified Nurse-Midwife Really Is
The word “midwife” often carries outdated assumptions. Some imagine informal training or limited medical authority. Midwives are sometimes misunderstood as ‘just doulas’ or imagined in a vintage, candlelit birth scene. In reality, Certified Nurse-Midwives (CNMs) are advanced practice medical providers, working within hospital-based teams.
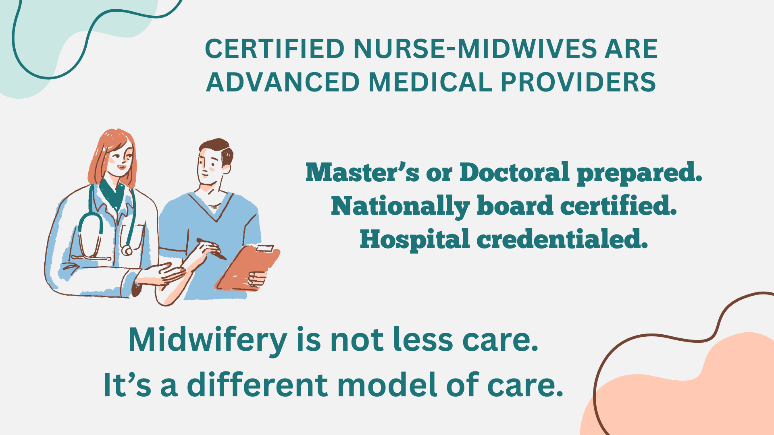
A CNM typically completes:
- A Bachelor of Science in Nursing (BSN)
- RN licensure
- A Master’s or Doctoral degree in Nurse-Midwifery (an additional 2–4 years)
- National board certification
- Ongoing continuing education and clinical competency requirements
In total, this often represents 6–8+ years of higher education and extensive clinical training.
CNMs are licensed to:
- Manage pregnancies independently
- Provide full prenatal, labor, birth, and postpartum care
- Identify complications early
- Consult and collaborate with obstetricians when medical or surgical intervention is needed
- Many CNMs are surgically trained and first assist on c-sections.
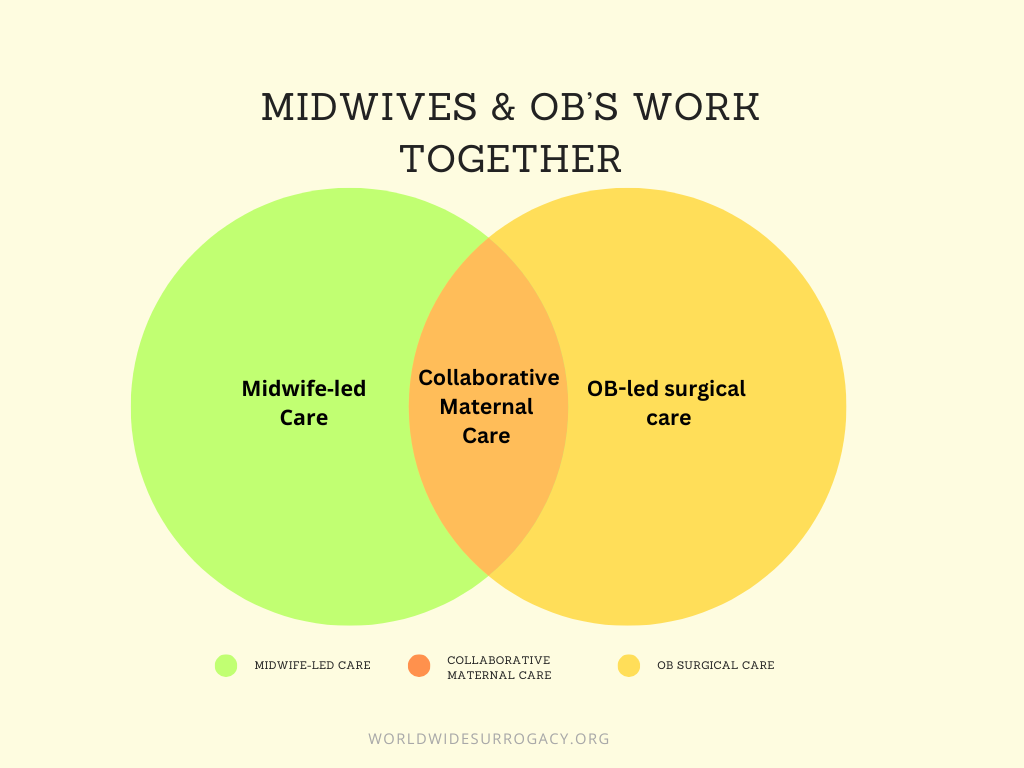
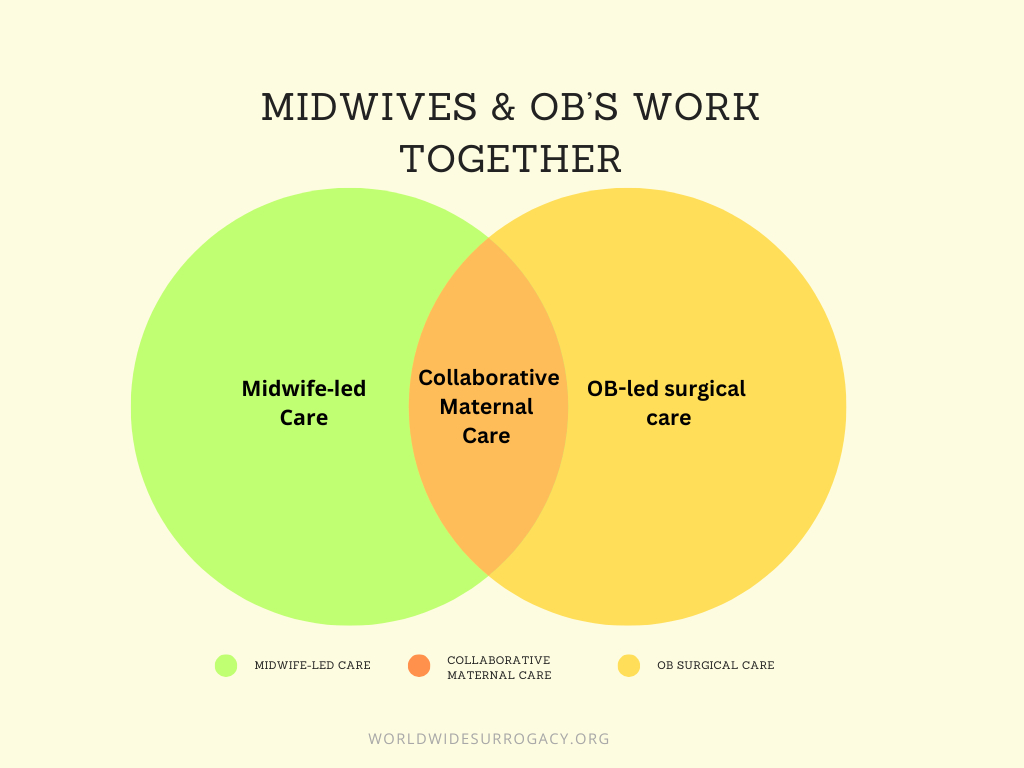
Importantly, in modern medical systems, OB-GYNs do not supervise CNMs. Instead, they work in collaborative care models, practicing as colleagues within clearly defined scopes of care.
There are clear clinical guidelines within every practice that determine:
- What CNMs manage independently
- What requires collaborative management
- What is physician-only care (which is relatively rare and typically involves higher-risk complications)
This structure is not casual. It is evidence-based and safety-driven, and leads to more integrated and comprehensive care.
IVF Pregnancies & Risk
Another understandable concern is that IVF pregnancies are automatically “high risk.” While IVF can be associated with certain increased risks, many surrogate pregnancies remain medically low-risk throughout gestation.
In hospital-based collaborative practices, choosing a CNM does not mean reducing medical oversight. It means:
- Hospital delivery
- Access to surgical teams
- Immediate physician involvement if needed
- Seamless transition of care if complications arise
In many ways, it is team-based care — not alternative care. For many pregnancies, midwives lead routine prenatal and labor care, while obstetricians are readily available for surgical or higher-risk situations.In some collaborative practices, patients do not have the option to request OB-only delivery, because the model itself is built around shared care. This approach is intentional, reflecting on how many modern hospital maternity practices are structured.
My Own Experience: OB Care vs. Midwifery Care
My perspective on this is both professional and deeply personal.
I delivered my oldest daughter under traditional OB care. It was safe, and I’m grateful for that. But much of my labor felt clinical and fragmented. My OB primarily came in during the final phase of delivery. Until then, I labored largely with nursing staff.
With my second daughter, I chose a midwives practice. The difference was profound. My midwife was present, hands-on, and actively coaching me through every stage. I felt guided, supported, and deeply cared for — not just medically managed. My recovery was noticeably smoother, and I attribute much of that to the way she coached positioning, pushing, and pacing throughout labor.
“That experience reshaped my understanding of what birth support could look like.”
The quality of care and support I received played a significant role in my decision to pursue surrogacy, and without that experience, I don’t believe I would have felt ready.
Carrying as a Surrogate — and Choosing Midwife Care Again
When I later carried a surrogate pregnancy through Women’s Health Associates and delivered at Yale, I chose the same midwives practice where I had delivered my second daughter.
My intended parents initially had concerns. And I understood them. IVF pregnancies carry emotional gravity. They had invested so much already — financially, medically, and emotionally.
So we talked through it.
I explained the collaborative structure. I explained that OBs and midwives work together. I explained that hospital delivery meant immediate escalation if needed. Once they understood that midwifery care did not mean reduced medical access, they supported my decision.
During that surrogate pregnancy, my IPs grew so grateful for the care they also had. What stood out was how intentionally my midwives included my intended parents. They took time to explain what was happening in real time, answered questions thoughtfully, and made sure the IPs felt seen and involved throughout the process. They didn’t just care for me clinically — they cared for the experience as a whole. That level of communication and inclusion created a sense of shared trust in the room, which mattered deeply in a surrogacy journey.
During my labor, a C-section ultimately became medically necessary. When that happened, the transition was seamless. An OB performed the surgery, while my midwife stayed with me — even in the operating room. She remained by my side through the entire procedure.
“What struck me most was this: I didn’t have less care because I chose a midwife. I had more. I had surgical expertise and continuous emotional support at the same time.”
Why This Conversation Matters in Surrogacy
Surrogacy requires extraordinary trust on both sides. Intended parents are entrusting someone with their future child. A surrogate is entrusting her body and health to carry that child safely.
When a surrogate chooses a CNM within a hospital-based, collaborative practice, she is not rejecting medical safety. She is choosing a model of care that feels supportive, attentive, and aligned with her prior birth experiences.
And ultimately, she is the one assuming the physical risk of pregnancy and birth.
That does not diminish the voice of intended parents. It simply acknowledges reality. In ethical surrogacy partnerships, decisions are made through open dialogue, education, and mutual respect — but bodily autonomy remains with the person carrying the pregnancy.
When Intended Parents understand: The education and rigor behind certified nurse-midwife training. The collaborative care structure between CNMs and OBs. The safety protocols built into hospital-based midwifery care. The clear guidelines for transitioning to physician-led care when needed.
A Shared Goal
At the end of the day, OB-led care and CNM-led care within hospital systems share the same goal: a healthy baby and a healthy surrogate.
The difference between these models of care is often not about safety, but about style of care, continuity, and philosophy of support. In surrogacy, the strongest partnerships are built on informed trust, communication, and shared understanding. When intended parents and surrogates approach these conversations with openness and education, they create space for both safety and empowerment. That balance is at the heart of what surrogacy is meant to be.
Get the Latest Updates
Categories